Georgia Marianthe Mesbouris takes a moment to herself before a follow-up procedure at Sunnybrook.
One weekend in August 2020, on a morning when Georgia Marianthe Mesbouris and her family were planning to leave for a family vacation, the 42-year-old resident of Scarborough, Ont., woke up with an incredible pain at the back of her neck. Knowing how much this vacation meant to her kids, she took a pain reliever and hoped the throbbing and sensation of burning hot ears would go away.
It didn’t.
Georgia, a mother of two and a tech expert on a national TV channel, considers herself a healthy person. “I don’t have high blood pressure. I don’t smoke. I [rarely] drink,” she says. So it was a complete shock when – after a trip to the emergency room – she was told that the pain she was experiencing was the result of two aneurysms in her brain.
One was small, but the other was very large. Aneurysms occur when a blood vessel wall weakens and bulges out, and the largest ones, called “giant aneurysms,” are typically no more than 2.5 centimetres across. Georgia’s was 3.5 centimetres long – one of the biggest the team at Sunnybrook had ever seen.
As long as the aneurysms remained in her head, Georgia’s life was at risk. One quarter of people with a ruptured aneurysm die within 24 hours, while another 25 per cent die within six months. For those who survive, many are left with permanent neurological damage.
Fortunately, Georgia’s care was in the hands of a Sunnybrook neurosurgeon whose expertise and ingenuity led to a novel approach to treatment that saved her life.
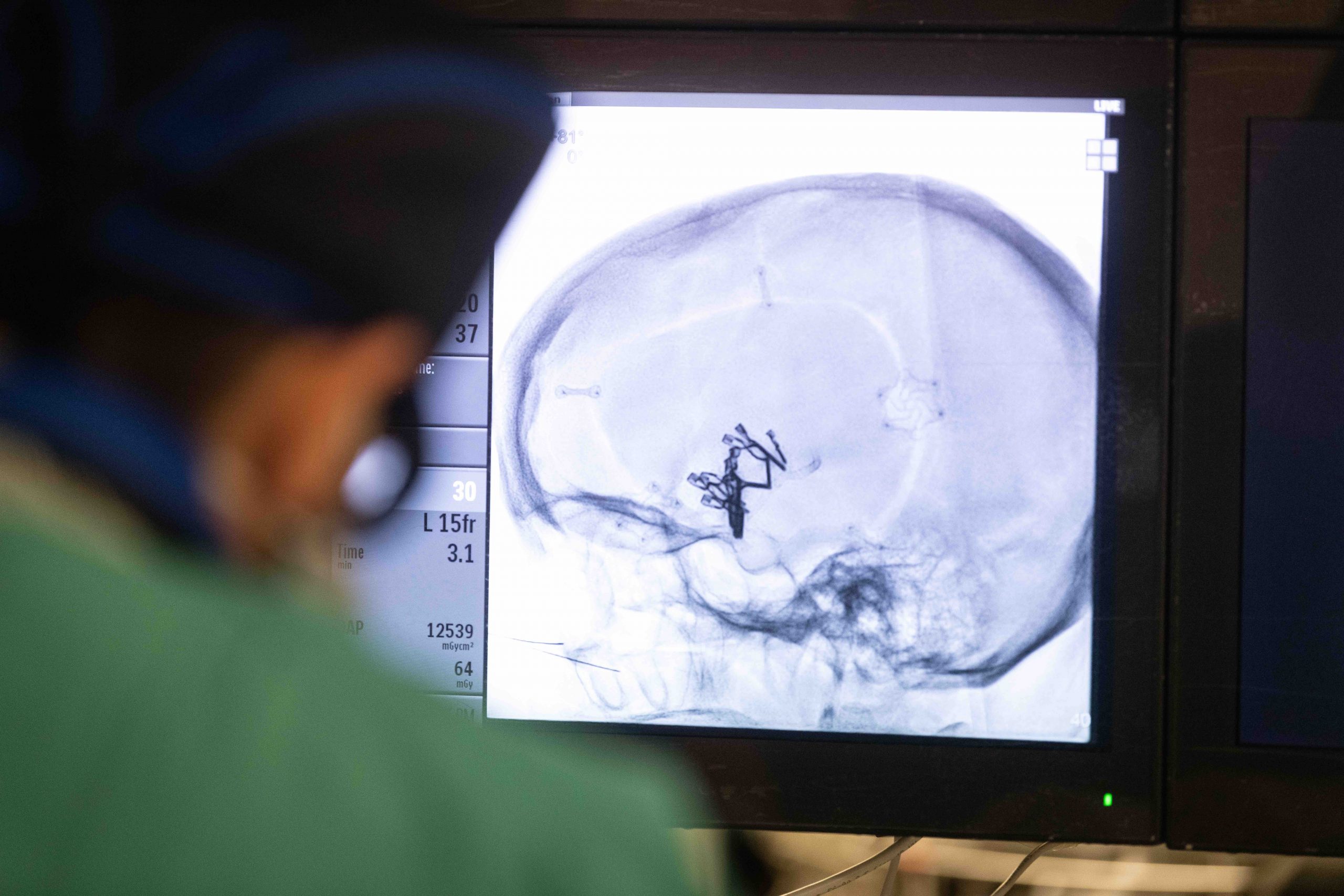
An X-ray shows the metal clips in Georgia’s brain following her crainotomy.
A problem with no easy solution
When faced with an aneurysm of this size, Sunnybrook neurosurgeon Dr. Leo da Costa knew he needed to come up with a unique treatment plan. Most aneurysms are berry-shaped, called saccular. But in Georgia’s case, the aneurysm was what’s called fusiformed – wide in the middle and tapered at both ends.
Another complication was that the larger aneurysm was located in the left hemisphere of Georgia’s brain, in the middle cerebral artery. This artery is responsible for providing much of the blood flow to the hemisphere, including the area of the brain responsible for speech. A rupture could have been devastating for Georgia, but she could not be treated using routine techniques.
“The easiest treatment for such large aneurysms is to close the vessel, which was not an option in this case. She could have a stroke on the left side of the brain and be paralyzed on the right side and unable to speak,” says Dr. da Costa, medical director of Sunnybrook’s Centre for Neurovascular Intervention.
Georgia says it was “surreal” to learn that her medical condition could be fatal or debilitating. But she felt hopeful that she would come through it all.
“My husband turned to me and he held my hand and [said], ‘Don’t die.’ So I told him, ‘I’m not going to die.’”
The neurovascular team’s initial treatment for Georgia was a craniotomy – brain surgery to reconstruct the affected blood vessel with metal clips. But while surgery was successful and Georgia went home, a month later an angiogram showed the aneurysm had grown again.
With Georgia’s life once again in jeopardy, Dr. da Costa decided that the situation called for another approach involving flow diverter stents. These special, tiny stents are made of mesh with very fine holes that change the way the blood flows around a vessel.
“If you imagine a tunnel, the blood goes mostly inside, and the [aneurysm] outside will slowly clot and shrink,” explains Dr. da Costa.
The problem with this approach was that Georgia’s aneurysm was far too long for these stents.
So, Dr. da Costa decided to try something unprecedented. He would telescope three miniscule stents into one another to bridge the distance of Georgia’s aneurysm.
Sunnybrook neurosurgeon Dr. Leo da Costa.
A unique approach
On October 2, 2020, Dr. da Costa and his team accessed Georgia’s brain through a small incision in her groin. Using a combination of catheters and wires, he navigated the tiny stents through her aorta and into the brain vessels where the aneurysm was located.
Dr. da Costa placed one stent from the edge of the healthy area of the blood vessel into the aneurysm, then placed another just inside that one to extend into the middle part of the aneurysm. Finally, a third stent was placed to complete the “bridge” to the other side.
“This has not been done before using these small stents; [we] were the first globally to telescope three flow diverters to successfully treat a small vessel middle cerebral artery aneurysm,” Dr. da Costa says.
In total, the surgery was just over an hour. Georgia woke up to hear a nurse complimenting her toenail polish. “That made me laugh, and when I laughed, they exclaimed, ‘She’s awake!’” she recalls.
She was released from the hospital shortly after the surgery and is recovering well. Last Christmas, Georgia sent Dr. da Costa a video with her two kids, thanking him for all he’d done to save her life.
“He’s so modest,” says Georgia. “He responded, ‘It wasn’t me. It was all you.’”
Less invasive and more efficient

Georgia and her children enjoy a sunny day in the park.
Dr. da Costa says the procedure will have a significant impact on how his team handles difficult aneurysms.
“Until very recently, open surgery was often the safest option for these very large aneurysms, and the procedures are often complex,” he says. “Finding out that we can add one very small stent to the other in a chain to cover longer distances will allow us to treat these aneurysms in a much less invasive and efficient manner.”
In fact, after Georgia’s treatment, Dr. da Costa said they did another similar one, using the same technique, and he is convinced more and more cases will be done in a similar fashion worldwide. That patient also did well and was discharged the next morning.
Dr. da Costa says that his team’s personalized and precise treatments work hand-in-hand with the constant evolution of technology in this space.
“Many improvements in existing devices and new, disruptive technology are launched every year, allowing us to push the boundaries of what can be treated and how we do it.”